Locametz
Generic name: gallium ga 68 gozetotide
Dosage form: injection, powder, lyophilized, for solution
Medically reviewed by A Ras MD. Last updated on Apr 1, 2022.
What is Locametz
Locametz, after radiolabeling with gallium-68, is indicated for positron emission tomography (PET) of prostate-specific membrane antigen (PSMA)-positive lesions in men with prostate cancer
INDICATIONS AND USAGE
- with suspected metastasis who are candidates for initial definitive therapy.
- with suspected recurrence based on elevated serum prostate-specific antigen (PSA) level.
- for selection of patients with metastatic prostate cancer, for whom lutetium Lu 177 vipivotide tetraxetan PSMA-directed therapy is indicated.
DOSAGE AND ADMINISTRATION
Radiation Safety – Drug Handling
 After reconstitution and radiolabeling of Locametz, the vial contains gallium Ga 68 gozetotide injection. Handle the gallium Ga 68 gozetotide injection with appropriate safety measures to minimize radiation exposure.Use waterproof gloves, effective radiation shielding, and other appropriate safety measures when preparing and handling gallium Ga 68 gozetotide injection.
After reconstitution and radiolabeling of Locametz, the vial contains gallium Ga 68 gozetotide injection. Handle the gallium Ga 68 gozetotide injection with appropriate safety measures to minimize radiation exposure.Use waterproof gloves, effective radiation shielding, and other appropriate safety measures when preparing and handling gallium Ga 68 gozetotide injection.
Radiopharmaceuticals should be used by or under the control of healthcare providers who are qualified by specific training and experience in the safe use and handling of radionuclides, and whose experience and training have been approved by the governmental agency authorized to license the use of radionuclides.¶
Recommended Dosage
In adults, the recommended amount of radioactivity to be administered for PET is 111 MBq to 259 MBq (3 mCi to 7 mCi) by slow intravenous injection.
Patient Preparation
Advise patients to be well hydrated prior to gallium Ga 68 gozetotide injection administration and to void immediately prior to and frequently during the first hours after image acquisition to reduce radiation exposure.
Drug Preparation
Locametz allows the direct preparation of gallium Ga 68 gozetotide injection with the eluate from one of the following generators (see below for specific instructions for use with each generator):
- Eckert & Ziegler GalliaPharm germanium-68/gallium-68 (68Ge/68Ga) generator
- IRE ELiT Galli Eo germanium-68/gallium-68 (68Ge/68Ga) generator
The instructions for use provided by the germanium-68/gallium-68 generator manufacturer should also be followed.
Prepare gallium Ga 68 gozetotide injection according to the following aseptic procedure:
a. Use suitable shielding to reduce radiation exposure.
b. Wear waterproof gloves.
c. Flip the cap off the Locametz vial and swab the septum with an appropriate antiseptic, then allow the septum to dry.
d. Pierce the Locametz vial septum with a sterile needle connected to a 0.2-micron sterile air venting filter to maintain atmospheric pressure within the vial during the reconstitution process.
e. Place the Locametz vial in a lead shield container.
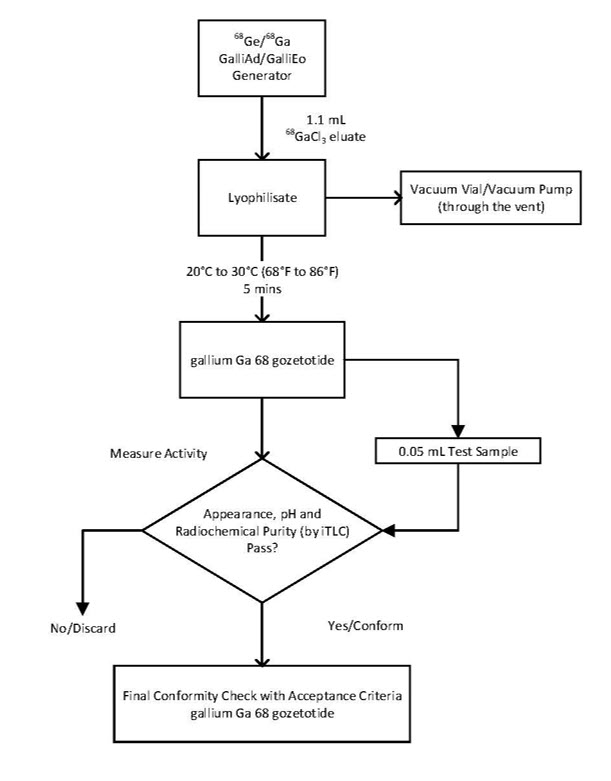
f. Follow the generator-specific procedures below. Schematic diagrams are provided in Figures 1 and 2.
Preparation with Eckert & Ziegler GalliaPharm Generator
1) Connect the male luer of the outlet line of the generator to a sterile elution needle (size 21G to 23G).
2) Connect the Locametz vial directly to the outlet line of the generator by pushing the elution needle through the rubber septum.
3) Elute directly from the generator into the Locametz vial.
4) Perform the elution manually or by means of a pump according to the generator instructions for use.
5) Reconstitute the lyophilized powder with 5 mL of the eluate.
6) At the end of the elution, disconnect the Locametz vial from the generator by removing the elution needle and the vent needle with the 0.2 micron sterile air venting filter from the rubber septum. Then, invert Locametz vial once and place it upright.
7) Incubate the Locametz vial upright between 20°C to 30°C (68°F to 86°F) for at least 5 minutes without agitation or stirring.
8) After 5 minutes, assay the vial containing the gallium Ga 68 gozetotide injection for total radioactivity using a dose calibrator, calculate the radioactivity concentration and record the result.
9) After radiolabeling, gallium Ga 68 gozetotide injection may be diluted with Sterile Water for Injection, USP or 0.9% Sodium Chloride Injection, USP up to a final volume of 10 mL.
10) Perform quality controls according to the recommended methods in order to check compliance with the specifications.
11) Store the Locametz vial containing the gallium Ga 68 gozetotide injection upright in a lead shield container below 30°C (86°F) until use.
12) After the addition of gallium-68 chloride to the Locametz vial, use gallium Ga 68 gozetotide injection within 4 hours.
Preparation with IRE ELiT Galli Eo Generator
1) Connect the male luer of the outlet line of the generator to a sterile elution needle (size 21G to 23G).
2) Connect the Locametz vial directly to the outlet line of the generator by pushing the elution needle through the rubber septum.
3) Connect the Locametz vial through the vent needle with 0.2 micron sterile air venting filter to a vacuum vial (25 mL minimum volume) by means of a sterile needle (size 21G to 23G) or to a vacuum pump to start the elution.
4) Elute directly from the generator into the Locametz vial.
5) Reconstitute the lyophilized powder with 1.1 mL of the eluate.
6) At the end of the elution, first withdraw the sterile needle from the vacuum vial or disconnect the vacuum pump in order to establish atmospheric pressure into the Locametz vial, then disconnect the vial from the generator by removing both the elution needle and the vent needle with the 0.2 micron sterile air venting filter needle from the rubber septum. Inversion of the Locametz vial is not needed.
7) Incubate the Locametz vial upright between 20°C to 30°C (68°F to 86°F) for at least 5 minutes without agitation or stirring.
8) After 5 minutes, assay the vial containing the gallium Ga 68 gozetotide injection for total radioactivity using a dose calibrator, calculate the radioactivity concentration and record the result.
9) After radiolabeling, gallium Ga 68 gozetotide injection may be diluted with Sterile Water for Injection, USP or 0.9% Sodium Chloride Injection, USP up to a final volume of 10 mL.
10) Perform quality controls according to the recommended methods in order to check compliance with the specifications.
11) Store the Locametz vial containing the gallium Ga 68 gozetotide injection upright in a lead shield container below 30°C (86°F) until use.
12) After the addition of gallium-68 chloride to the Locametz vial, use gallium Ga 68 gozetotide injection within 4 hours.
Figure 1. Preparation with Eckert & Ziegler GalliaPharm Generator
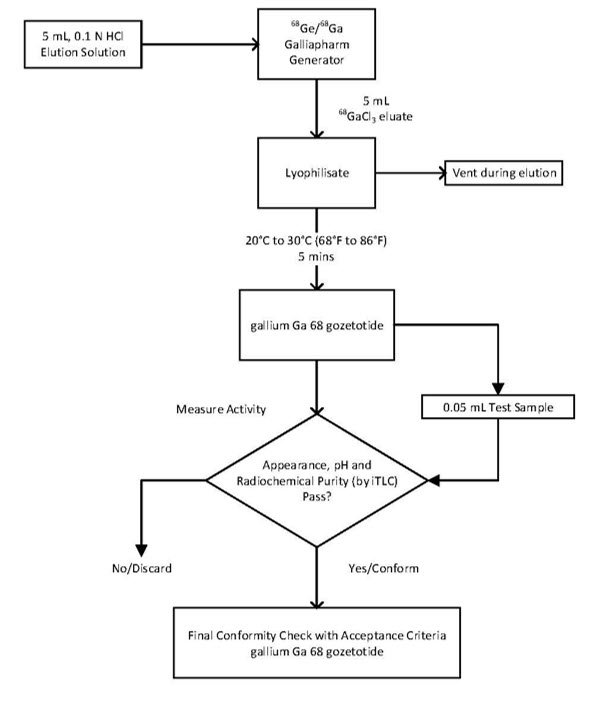
Figure 2. Preparation with IRE ELiT Galli Eo Generator
Specifications and Quality Control
Perform the quality controls in Table 1 behind a lead glass shield for radioprotection purposes.
| Test | Acceptance criteria | Method |
| Appearance | Clear, colorless, and free from particulate matter | Visual inspection |
| pH | 3.2 to 6.5 | pH-indicator strips |
| Radiochemical Purity | gallium Ga 68 gozetotide ≥ 95% Non-complexed gallium-68 species ≤ 5% |
Instant thin-layer chromatography (ITLC, see details below) |
Determine radiochemical purity of gallium Ga 68 gozetotide injection by performing instant thin-layer chromatography (ITLC).
Perform ITLC using ITLC SG strips and using ammonium acetate 1M: Methanol (1:1 V/V) as mobile phase.
ITLC Method
a. Develop the ITLC SG strip for a distance of 6 cm from the point of application (i.e., to 7 cm from the bottom of the ITLC strip).
b. Scan the ITLC SG strip with a radiometric ITLC scanner.
c. Calculate radiochemical purity by integration of the peaks on the chromatogram. Do not use the reconstituted product if the percentage (%) of non-complexed gallium-68 species is higher than 5%.
The retention factor (Rf) specifications are as follows:
- Non-complexed gallium-68 species, Rf = 0 to 0.2;
- Gallium Ga 68 gozetotide, Rf = 0.8 to 1.
Administration
a. Use aseptic technique and radiation shielding when withdrawing and administering gallium Ga 68 gozetotide injection.
b. Calculate the necessary volume to administer based on calibration time and required dose.
c. Inspect the prepared gallium Ga 68 gozetotide injection for particulate matter and discoloration behind a lead glass shield for radioprotection purposes. Use only solutions that are clear, colorless, and free from particulate matter.
d. Using a single-dose syringe fitted with a sterile needle (size 21G to 23G) and protective shielding, aseptically withdraw the prepared gallium Ga 68 gozetotide injection.
e. Verify the total radioactivity in the syringe with a dose calibrator immediately before and after gallium Ga 68 gozetotide injection administration to the patient. The dose calibrator must be calibrated with NIST traceable standards.
f. After injection of gallium Ga 68 gozetotide, administer an intravenous flush of sterile 0.9% Sodium Chloride Injection, USP to ensure full delivery of the dose.
g. Dispose of any unused gallium Ga 68 gozetotide injection in a safe manner in compliance with applicable regulations.
h. If clinically necessary, a diuretic expected to act within the uptake time period may be administered at the time of radiotracer injection to potentially decrease artifact from radiotracer accumulation in the urinary bladder and ureters.
Image Acquisition
Begin PET scanning 50 minutes to 100 minutes after the intravenous administration of gallium Ga 68 gozetotide injection. Patients should void immediately prior to image acquisition and image acquisition should begin at the mid-thighs and proceed cranially to the skull base or skull vertex. Adapt imaging techniques according to the equipment used and patient characteristics in order to obtain the best image quality possible.
Image Interpretation
Gallium Ga 68 gozetotide binds to PSMA. Based on the intensity of the signals, PET images obtained using gallium Ga 68 gozetotide injection indicate the presence of PSMA in tissues.
Imaging Prior to Initial Definitive or Suspected Recurrence Therapy
Lesions should be considered suspicious if uptake is greater than physiologic uptake in that tissue or greater than adjacent background if no physiologic uptake is expected. Tumors that do not bear PSMA will not be visualized. Increased uptake in tumors is not specific for prostate cancer.
Imaging to Select Patients for Lutetium Lu 177 Vipivotide Tetraxetan Therapy
For patient selection, interpret Locametz PET in conjunction with patients’ clinical history and imaging from other modalities, including diagnostic anatomical imaging in clinically relevant regions, such as the chest, abdomen, and pelvis. On Locametz PET images, compare uptake of gallium Ga 68 gozetotide at sites of suspected prostate cancer (lesions) with uptake in normal liver. Lesions should be considered positive if gallium Ga 68 gozetotide uptake is greater than normal liver and negative if gallium Ga 68 gozetotide uptake is less than or equal to normal liver.
Patients should be considered eligible for lutetium Lu 177 vipivotide tetraxetan therapy if at least one tumor lesion is positive and all lesions on anatomical imaging larger in short axis than size criteria are also positive [size criteria: organs ≥ 1 cm, lymph nodes ≥ 2.5 cm, bones (soft tissue component) ≥ 1 cm]. Patients should be considered ineligible for lutetium Lu 177 vipivotide tetraxetan therapy if all lesions are negative or any one lesion larger than size criteria is negative.
The interpretation of Locametz PET may differ depending on imaging readers.
For therapeutic information, refer to the prescribing information for lutetium Lu 177 vipivotide tetraxetan.
Radiation Dosimetry
Estimated radiation absorbed doses per injected activity for organs and tissues of 13 adult male patients with an early stage of disease following an intravenous bolus of gallium Ga 68 gozetotide injection are shown in Table 2.
The effective radiation dose resulting from the administration of 259 MBq (7 mCi) is 4.4 mSv. The radiation doses for this administered dose to the critical organs, which are the kidneys, urinary bladder, and spleen, are 96.2 mGy, 25.4 mGy, and 16.8 mGy, respectively.
These radiation doses are for gallium Ga 68 gozetotide injection alone. If CT or a transmission source are used for attenuation correction, the radiation dose will increase by an amount that varies by technique.
| Absorbed dose (mGy/MBq) | ||
| Organ | Mean | SD |
| Adrenals | 0.0156 | 0.0014 |
| Brain | 0.0104 | 0.0011 |
| Breasts | 0.0103 | 0.0011 |
| Gallbladder | 0.0157 | 0.0012 |
| Lower Colon | 0.0134 | 0.0009 |
| Small Intestine | 0.014 | 0.002 |
| Stomach | 0.0129 | 0.0008 |
| Heart | 0.012 | 0.0009 |
| Kidneys | 0.3714 | 0.0922 |
| Liver | 0.0409 | 0.0076 |
| Lungs | 0.0111 | 0.0007 |
| Muscle | 0.0103 | 0.0003 |
| Pancreas | 0.0147 | 0.0009 |
| Red Marrow | 0.0114 | 0.0016 |
| Skin | 0.0091 | 0.0003 |
| Spleen | 0.065 | 0.018 |
| Testes | 0.0111 | 0.0006 |
| Thymus | 0.0105 | 0.0006 |
| Thyroid | 0.0104 | 0.0006 |
| Urinary Bladder | 0.0982 | 0.0286 |
| Total Body | 0.0143 | 0.0013 |
| Effective Dose (mSv/MBq) | 0.0169 | 0.0015 |
DOSAGE FORMS AND STRENGTHS
Locametz is a kit for the preparation of gallium Ga 68 gozetotide injection supplied in a multiple-dose vial containing 25 micrograms of gozetotide as a white lyophilized powder.
Gallium-68 is obtained from one of the following generators:
- Eckert & Ziegler GalliaPharm (Ge 68/Ga 68) generator
- IRE ELiT Galli Eo (Ge 68/Ga 68) generator
After radiolabeling with gallium-68, each vial contains a sterile, clear, colorless solution free from the particulate matter of gallium Ga 68 gozetotide at an activity of up to 1,369 MBq (37 mCi) in up to 10 mL at the calibration date and time.¶
CONTRAINDICATIONS
None.
WARNINGS AND PRECAUTIONS
Risk for Misinterpretation
Image interpretation errors can occur with Locametz PET. Negative imaging does not rule out the presence of prostate cancer and positive imaging does not confirm the presence of prostate cancer. Gallium Ga 68 gozetotide uptake is not specific for prostate cancer and may occur with other types of cancer as well as non-malignant processes, such as Paget’s disease, fibrous dysplasia, and osteophytosis. Clinical correlation, which may include histopathological evaluation of the suspected prostate cancer site, is recommended.
Imaging Prior to Initial Definitive or Suspected Recurrence Therapy
The performance of Locametz for imaging of biochemically recurrent prostate cancer seems to be affected by serum PSA levels and by site of disease. The performance of Locametz for imaging of metastatic pelvic lymph nodes prior to initial definitive therapy seems to be affected by Gleason score.
Imaging to Select Patients for Lutetium Lu 177 Vipivotide Tetraxetan Therapy
The interpretation of Locametz PET may differ depending on imaging readers. Locametz PET interpretations to select patients for lutetium Lu 177 vipivotide tetraxetan therapy may be more consistent when judging gallium Ga 68 gozetotide uptake in any one tumor lesion compared to judging uptake for all lesions larger than size criteria [see Clinical Studies (14.3)]. Multidisciplinary consultation to select patients for lutetium Lu 177 vipivotide tetraxetan therapy is recommended, particularly for Locametz imaging that a single reader finds borderline or difficult to interpret, or when patient eligibility hinges only on judgment of gallium Ga 68 gozetotide uptake for all lesions larger than size criteria.
Radiation Risk
Gallium Ga 68 gozetotide contributes to the patient’s overall long-term cumulative radiation exposure. Long-term cumulative radiation exposure is associated with an increased risk of cancer. Ensure safe handling to minimize radiation exposure to the patient and health care workers. Advise patients to be well hydrated prior to gallium Ga 68 gozetotide injection administration and to void immediately prior to and frequently during the first hours after image acquisition to reduce radiation exposure.
ADVERSE REACTIONS
Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice.
The safety of Locametz has been established based on three prospective studies of gallium Ga 68 gozetotide in patients with prostate cancer.. Adverse reactions from these studies are reported below.
In the PSMA-PreRP and PSMA-BCR studies using another formulation of gallium Ga 68 gozetotide, nine-hundred sixty (960) patients received one dose of gallium Ga 68 gozetotide intravenously with the amount (mean ± SD) of radioactivity 188.7 ± 40.7 MBq (5.1 ± 1.1 mCi).. The most commonly reported adverse reactions were nausea, diarrhea and dizziness, occurring at a rate of < 1%.
In the VISION study, one thousand and three (1003) patients received one dose of gallium Ga 68 gozetotide intravenously with the amount of radioactivity 167.1 ± 23.1 MBq (4.52 ± 0.62 mCi) [see Clinical Studies (14.3)]. Adverse reactions occurring at ≥ 0.5% in patients with metastatic prostate cancer who received gallium Ga 68 gozetotide injection are presented in Table 3.
| Adverse Reactions | Gallium Ga 68 Gozetotide Injection N = 1003 n (%) |
| General disorders | |
| Fatigue | 12 (1.2) |
| Gastrointestinal disorders | |
| Nausea | 8 (0.8) |
| Constipation | 5 (0.5) |
| Vomiting | 5 (0.5) |
Adverse reactions occurring at a rate of < 0.5% in the VISION study were diarrhea, dry mouth, injection site reactions, including injection site hematoma and injection site warmth and chills.
DRUG INTERACTIONS
Androgen Deprivation Therapy and Other Therapies Targeting the Androgen Pathway
Androgen deprivation therapy (ADT) and other therapies targeting the androgen pathway, such as androgen receptor antagonists, can result in changes in the uptake of gallium Ga 68 gozetotide in prostate cancer. The effect of these therapies on performance of Locametz PET has not been established.
USE IN SPECIFIC POPULATIONS
Pregnancy
Risk Summary
Locametz is not indicated for use in females. There are no available data with gallium Ga 68 gozetotide use in pregnant women to evaluate for a drug-associated risk of major birth defects, miscarriage, or adverse maternal or fetal outcomes. All radiopharmaceuticals, including Locametz have the potential to cause fetal harm depending on the fetal stage of development and the magnitude of radiation dose. Animal reproduction studies have not been conducted with gallium Ga 68 gozetotide.
Lactation
Risk Summary
Locametz is not indicated for use in females. There are no data on the presence of gallium Ga 68 gozetotide in human milk, the effect on the breastfed infant, or the effect on milk production.
Pediatric Use
The safety and effectiveness of gallium Ga 68 gozetotide in pediatric patients have not been established.
Geriatric Use
The efficacy of Locametz in geriatric patients with prostate cancer is based on data from three prospective studies [see Clinical Studies (14)].
Of the total number of subjects in the PSMA-PreRP and PSMA-BCR studies, 691 of 960 (72%) patients were 65 years of age and older while 195 (20%) were 75 years of age and older.
Of the total number of subjects in the VISION study, 752 of 1003 (75%) patients were 65 years of age and older while 284 (28%) were 75 years of age and older.
The efficacy and safety profiles of gallium Ga 68 gozetotide appeared similar in younger adult and geriatric patients with prostate cancer and other reported clinical experience has not identified differences in responses between the elderly and younger patients.
OVERDOSAGE
In the event of an overdose of gallium Ga 68 gozetotide, reduce the radiation absorbed dose to the patient where possible by increasing the elimination of the radioactivity from the body by hydration and frequent bladder voiding. A diuretic might also be considered. If possible, an estimate of the effective radiation dose exposure to the patient should be made.
DESCRIPTION
Chemical Characteristics
Locametz (kit for the preparation of gallium Ga 68 gozetotide injection) is a sterile, radioactive diagnostic agent for intravenous administration after radiolabeling. Each vial contains 25 micrograms of gozetotide, 1 mg gentisic acid, 78 mg of sodium acetate trihydrate, and 40 mg sodium chloride. Gozetotide is also known as PSMA-11.
After reconstitution and radiolabeling of Locametz, the vial contains gallium Ga 68 gozetotide injection at a radioactivity of up to 1,369 MBq (37 mCi) in up to 10 mL at calibration date and time. The vial also contains hydrochloric acid derived from the gallium-68 chloride solution. Gallium Ga 68 gozetotide injection has a pH between 3.2 to 6.5.
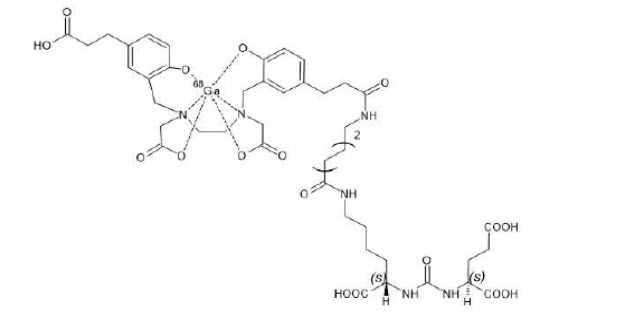
Gallium Ga 68 gozetotide is a urea based peptidomimetic that has a covalently bound chelator (HBED-CC). The peptide has amino acid sequence OH-Glu-CO-Lys(Ahx-CC-HBED)-OH.
Gallium Ga 68 gozetotide has a molecular weight of 1011.91 g/mol. The chemical structure is shown in Figure 3.
Figure 3. Chemical Structure of Gallium Ga 68 Gozetotide
Physical Characteristics
Gallium-68 decays with a half-life of 68 minutes to stable zinc-68. Table 4 and Table 5 display the principle radiation emission data, and physical decay of gallium-68.
| Radiation/Emission | % Disintegration | Mean Energy (MeV) |
| beta+ | 88% | 0.8360 |
| beta+ | 1.1% | 0.3526 |
| Gamma | 178% | 0.5110 |
| Gamma | 3% | 1.0770 |
| X-ray | 2.8% | 0.0086 |
| X-ray | 1.4% | 0.0086 |
| Minutes | Fraction Remaining |
| 0 | 1 |
| 15 | 0.858 |
| 30 | 0.736 |
| 60 | 0.541 |
| 90 | 0.398 |
| 120 | 0.293 |
| 180 | 0.158 |
| 240 | 0.086 |
| 360 | 0.025 |
Radiation Attenuation
Table 6 displays the radiation attenuation by lead shielding of gallium-68.
| Shield Thickness (Pb) mm | Coefficient of Attenuation |
| 6 | 0.5 |
| 12 | 0.25 |
| 17 | 0.1 |
| 34 | 0.01 |
| 51 | 0.001 |
CLINICAL PHARMACOLOGY
Mechanism of Action
Gallium Ga 68 gozetotide binds to PSMA. It binds to cells that express PSMA, including malignant prostate cancer cells, which usually overexpress PSMA. Gallium-68 is a β+ emitting radionuclide that allows PET.
Pharmacodynamics
The relationship between gallium Ga 68 gozetotide plasma concentrations and successful imaging was not explored in clinical trials.
Pharmacokinetics
Distribution
Intravenously injected gallium Ga 68 gozetotide is cleared from the blood and is accumulated preferentially in the liver (15%), kidneys (7%), spleen (2%), and salivary glands (0.5%). Gallium Ga 68 gozetotide uptake is also seen in the adrenals and prostate. There is no uptake in the cerebral cortex or in the heart, and usually lung uptake is low.
Gozetotide exhibits a mean blood-to-plasma ratio (% CV) of 0.71 (26%), and is approximately 33% bound to human plasma proteins at 1 mcg/mL to 5 mcg/mL in vitro.
Elimination
A total of 14% of the injected dose is excreted in the urine in the first 2 hours post-injection.
In Vitro Drug Interaction Studies
CYP450 enzymes
Gozetotide is not a substrate of cytochrome P450 (CYP450) enzymes, not an inhibitor of CYP1A2, CYP2B6, CYP2C8, CYP2C19, CYP2D6 and CYP3A4, and not an inducer of CYP1A2, CYP2B6, and CYP3A4 in vitro.
Transporters
Gozetotide is not a substrate of BCRP, P-gp, MATE1, MATE2-K, OAT1, OAT3 or OCT2. Gozetotide is not an inhibitor of BCRP, P-gp, MATE1, MATE2-K, OAT1, OAT3, OATP1B1, OATP1B3, OCT1 or OCT2 in vitro.
NONCLINICAL TOXICOLOGY
Carcinogenesis, Mutagenesis, Impairment of Fertility
No studies on mutagenic, carcinogenic potential or fertility have been conducted with gallium Ga 68 gozetotide.
CLINICAL STUDIES
Imaging Prior to Initial Definitive Therapy
The efficacy of Locametz for PET of PSMA-positive lesions in men with prostate cancer with suspected metastasis who are candidates for initial definitive therapy has been established based on a study of another formulation of gallium Ga 68 gozetotide. Below is a display of the results of the prospective, open label study PSMA-PreRP (NCT03368547 and NCT02919111).
PSMA-PreRP
This two-center study enrolled 325 patients with biopsy-proven prostate cancer who were considered candidates for prostatectomy and pelvic lymph node dissection. All enrolled patients met at least one of the following criteria: serum PSA of at least 10 ng/mL, tumor stage cT2b or greater, or Gleason score greater than 6. Each patient received a single gallium Ga 68 gozetotide PET/CT or PET/MR from mid-thigh to skull base.
A total of 123 patients (38%) proceeded to standard-of-care prostatectomy and template pelvic lymph node dissection and had sufficient histopathology data for evaluation (evaluable patients). Three members of a pool of six central readers independently interpreted each PET scan for the presence of abnormal gallium Ga 68 gozetotide uptake in pelvic lymph nodes located in the common iliac, external iliac, internal iliac, and obturator subregions bilaterally as well as in any other pelvic location. The readers were blinded to all clinical information except for the history of prostate cancer prior to definitive treatment. Extrapelvic sites and the prostate gland itself were not analyzed in this study. For each patient, gallium Ga 68 gozetotide PET results and reference standard histopathology obtained from dissected pelvic lymph nodes were compared by region (left hemipelvis, right hemipelvis, and other).
For the 123 evaluable patients, the mean age was 65 years (range, 45 to 76 years), and 89% were white. The median serum PSA was 11.8 ng/mL. The summed Gleason score was 7 for 44%, 8 for 20%, and 9 for 31% of the patients, with the remainder of the patients having Gleason scores of 6 or 10.
Table 7 compares majority PET reads to pelvic lymph node histopathology results at the patient-level with region matching, such that at least one true positive region defines a true positive patient. As shown, approximately 24% of subjects studied were found to have pelvic nodal metastases based on histopathology (95% CI: 17, 32).
| Abbreviations: CI, confidence interval; PPV, positive predictive value; NPV, negative predictive value. aWith region matching where at least one true positive region defines a true positive patient. |
||||
| Histopathology | Predictive value % (95% CI) | |||
| Positive | Negative | |||
| PET Scan | Positive | 14 | 9 | PPV 61% (41, 81) |
| Negative | 16 | 84 | NPV 84% (79, 91) |
|
| Total | 30 | 93 | ||
| Diagnostic performance % (95% CI) | Sensitivity 47% (29, 65) |
Specificity 90% (84, 96) |
||
Among the pool of six readers, sensitivity ranged from 36% to 60%, specificity from 83% to 96%, the positive predictive value from 38% to 80%, and negative predictive value from 80% to 88%.
In an exploratory subgroup analysis based on summed Gleason score, there was a numerical trend toward more true positives in patients with Gleason score of 8 or higher compared to those with Gleason score of 7 or lower.
An exploratory analysis was performed to estimate the sensitivity and specificity for pelvic nodal metastasis detection in all scanned patients, including the patients who were lacking histopathology reference standard. An imputation method was used based on patient-specific factors. This exploratory analysis resulted in an imputed sensitivity of 47%, with a 95% confidence interval (CI) ranging from 38% to 55%, and an imputed specificity of 74%, with a 95% CI ranging from 68% to 80% for all patients imaged with gallium Ga 68 gozetotide PET.
Imaging Prior to Suspected Recurrence Therapy
The efficacy of Locametz for PET of PSMA-positive lesions in men with prostate cancer with suspected recurrence based on elevated serum PSA level has been established based on studies of another formulation of gallium Ga 68 gozetotide. Below is a display of the result of the prospective, open label study PSMA-BCR (NCT02940262 and NCT02918357).
PSMA-BCR
This two-center study enrolled 635 patients with biochemical evidence of recurrent prostate cancer after definitive therapy, defined by serum PSA of > 0.2 ng/mL more than 6 weeks after prostatectomy or by an increase in serum PSA of at least 2 ng/mL above nadir after definitive radiotherapy. All patients received a single gallium Ga 68 gozetotide PET/CT or PET/MR from mid-thigh to skull base. Three members of a pool of nine independent central readers evaluated each scan for the presence and regional location (20 subregions grouped into four regions) of abnormal gallium Ga 68 gozetotide uptake suggestive of recurrent prostate cancer. The readers were blinded to all clinical information other than type of primary therapy and most recent serum PSA level.
A total of 469 patients (74%) had at least one positive region detected by gallium Ga 68 gozetotide PET majority read. The distribution of gallium Ga 68 gozetotide PET positive regions was 34% bone, 25% prostate bed, 25% pelvic lymph node, and 17% extrapelvic soft tissue. Two hundred and ten patients had composite reference standard information collected in a PET positive region (evaluable patients), consisting of at least one of the following: histopathology, imaging (bone scintigraphy, CT, or MRI) acquired at baseline or within 12 months after gallium Ga 68 gozetotide PET, or serial serum PSA. Composite reference standard information for gallium Ga 68 gozetotide PET negative regions was not systematically collected in this study.
In the 210 evaluable patients, the mean age was 70 years (range, 49 to 88 years) and 82% were 65 years of age or older. White patients made up 90% of the group. The median serum PSA was 3.6 ng/mL. Prior treatment included radical prostatectomy in 64% and radiotherapy in 73%.
Of the 210 evaluable patients, 192 patients (91%) were found to be true positive in one or more regions against the composite reference standard (95% CI: 88%, 95%). Among the pool of nine readers used in the study, the proportion of patients who were true positive in one or more regions ranged from 82% to 97%. The prostate bed had the lowest proportion of true positive results at the region-level (76% versus 96% for non-prostate regions).
An exploratory analysis was also performed in which gallium Ga 68 gozetotide PET positive patients who lacked reference standard information were imputed using an estimated likelihood that at least one location-matched PET positive lesion was reference standard positive based on patient-specific factors. In this exploratory analysis, 340 of 475 patients (72%) were imputed as true positive in one or more regions (95% CI: 68%, 76%).
In another exploratory analysis using the same imputation approach for PET positive patients who lacked reference standard information, 340 of 635 patients (54%) were correctly detected as true positive (95% CI: 50%, 57%) among all BCR patients who received a PET scan, whether it was read as positive or negative. The likelihood of identifying a gallium Ga 68 gozetotide PET positive lesion in this study generally increased with higher serum PSA level. Table 8 shows the patient-level gallium Ga 68 gozetotide PET results stratified by serum PSA level. The mean time between PSA measurement and PET scan was 40 days with a range of 0 to 367 days. Percent PET positivity was calculated as the proportion of patients with a positive gallium Ga 68 gozetotide PET out of all patients scanned. Percent PET positivity includes patients determined to be either true positive or false positive as well as those in whom such determination was not made due to the absence of composite reference standard data.
| Abbreviations: PET, positron emission tomography; PSA, prostate-specific antigen; PSMA, prostate-specific membrane antigen; BCR, biochemical recurrence; TP, true positive; FP, false positive. a7 patients were excluded from this table due to protocol deviations. bPercent PET positivity: PET positive patients/total patients scanned. |
||||||
| PET-positive patients | ||||||
| PSA (ng/mL) | Total | TP | FP | Without reference standard | PET-negative patients | PET positivity %b (95% CI) |
| With reference standard | ||||||
| < 0.5 | 48 | 11 | 1 | 36 | 87 | 36% (27, 44) |
| 12 | ||||||
| ≥ 0.5 and < 1 | 44 | 15 | 3 | 26 | 35 | 56% (45, 67) |
| 18 | ||||||
| ≥ 1 and < 2 | 71 | 29 | 1 | 41 | 15 | 83% (75, 91) |
| 30 | ||||||
| ≥ 2 | 299 | 137 | 13 | 149 | 29 | 91% (88, 94) |
| 150 | ||||||
| Total | 462 | 192 | 18 | 252 | 166 | 74% (70, 77) |
| 210 | ||||||
Imaging to Select Patients for Lutetium Lu 177 Vipivotide Tetraxetan Therapy
The efficacy of Locametz for selecting patients for lutetium Lu 177 vipivotide tetraxetan therapy was evaluated in VISION (NCT03511664), a randomized (2:1), multicenter, open-label trial that evaluated lutetium Lu 177 vipivotide tetraxetan plus best standard of care (BSoC; N = 551) or BSoC alone (N = 280) in men with progressive metastatic castration resistant prostate cancer (mCRPC). Gallium Ga 68 gozetotide was used to identify PSMA-positive patients on PET imaging. Only PSMA-positive patients were eligible for randomization and receipt of lutetium Lu 177 vipivotide tetraxetan.
VISION
A total of 1003 adult male patients with mCRPC received gallium Ga 68 gozetotide by intravenous administration and underwent PET imaging at approximately 60 minutes (range, 50 to 100 minutes) after injection. Gallium Ga 68 gozetotide PET imaging was interpreted in conjunction with post-contrast CT and/or MRI of the chest, abdomen, and pelvis for all patients, and in addition to brain MRI and/or CT in patients with history of CNS metastasis.
Patients were males of median age 70 years (range, 40 to 94 years), white (87%), black or African American (7%) and Asian (2.4%), and had median baseline PSA levels of 74 ng/mL (range, 0 to 8995 ng/mL).
Gallium Ga 68 gozetotide PET and anatomical imaging was interpreted by one central reader who was blinded to clinical information and other PET and bone imaging. PSMA-positive (eligible) patients were defined as those having at least one tumor lesion with gallium Ga 68 gozetotide uptake greater than normal liver and all tumor lesions larger than size criteria with gallium Ga 68 gozetotide uptake greater than liver [short axis size criteria: organs ≥ 1 cm, lymph nodes ≥ 2.5 cm, bones (soft tissue component) ≥ 1 cm]. Of the patients evaluated by the central reader, 869 (87%) were found to be PSMA-positive (eligible) and 126 (13%) were found to be PSMA-negative (ineligible) for lutetium Lu 177 vipivotide tetraxetan therapy.
A reader sub-study evaluated imaging interpretation agreement. Among the 869 patients found eligible and 126 patients found ineligible for therapy, 75 and 50, respectively, were selected at random (total of 125). Gallium Ga 68 gozetotide PET and anatomical imaging from these 125 patients was interpreted by three additional central readers (re-readers) who were blinded to clinical information and other PET and bone imaging. Imaging from 20 of the 125 patients was also randomly selected to assess intra-reader reproducibility. The estimated inter-reader Fleiss κ was 0.60 (95% CI: 0.50, 0.70) across the three re-readers, while the estimated intra-reader Cohen κ was 0.78 (95% CI: 0.49, 0.99), 0.76 (95% CI: 0.46, 0.99) and 0.89 (95% CI: 0.67, 0.99) for each re-reader.
Given the observed levels of inter-reader agreement, patient’s PSMA interpretations were further evaluated by eligibility and eligibility sub-criteria. Of the 125 patients with four readers (reader and re-readers), at least one reader found the patient to be PSMA-negative for lutetium Lu 177 vipivotide tetraxetan therapy in 59 patients. All four readers agreed in 20 of the 59 patients (34% reader unanimity). Based on the sub-criteria involving evaluation of any one tumor lesion and evaluation of all lesions larger than size criteria, at least one reader found the patient to be PSMA-negative in 21 patients (43% reader unanimity) and 45 patients (16% reader unanimity), respectively.
HOW SUPPLIED/STORAGE AND HANDLING
How Supplied
Locametz is supplied as a kit for the preparation of gallium Ga 68 gozetotide injection in a carton of 1 vial (NDC# 69488-017-61).
Each multiple-dose vial contains 25 micrograms of gozetotide as white lyophilized powder packaged in a 10 mL type I Plus glass vial closed with a rubber stopper and sealed with a flip-off cap.
Storage and Handling
Before reconstitution, store at 2°C to 25°C (36°F to 77°F). Do not freeze.
After radiolabeling, store upright with an appropriate lead shielding to protect from radiation, below 30°C (86°F). Do not freeze. After radiolabeling, use within 4 hours.
This preparation is approved for use by persons under license by the Nuclear Regulatory Commission or the relevant regulatory authority of an Agreement State.
PATIENT COUNSELING INFORMATION
Adequate Hydration
Advise patients to be well hydrated prior to the administration of gallium Ga 68 gozetotide injection and urge them to urinate immediately prior to image acquisition and frequently during the first hours following administration to reduce radiation exposure [see Dosage and Administration (2.3), Warnings and Precautions (5.2)].
Distributed by:
Advanced Accelerator Applications USA, Inc.
Millburn, NJ 07041
© 2022 Advanced Accelerator Applications USA, Inc.
Locametz is a registered trademark of Novartis AG and/or its affiliates
T2022-16
PRINCIPAL DISPLAY PANEL
Locametz®
kit for the preparation of
gallium Ga 68 gozetotide injection
25 mcg per vial gozetotide
For Intravenous Use Only
Radiolabel with gallium-68 chloride before use
RX-Only
NDC 69488-017-61
Advanced Accelerator Applications USA, Inc. Millburn, NJ 07041